Underpinned by improved understanding of the molecular basis of melanoma and regulation of immune system [7], new effective targeted and immune therapies have transformed the management of patients with widespread melanoma metastases. Breslow thickness is not reported for melanoma in situ. The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). WebMelanoma in situ in contrast to Paget, melanoma is negative for cytokeratins, EMA and CEA. Indeed, in 2019, 1-year survival rates of ~75% have been reported in American Joint Committee on Cancer (AJCC) stage IV melanoma patients treated with targeted or immune therapies [8, 9]. A special tissue-sparing technique may be used for a large melanoma in situ, such as Mohs micrographic surgery or staged mapped excisions [2]. N Engl J Med. Slider with three articles shown per slide. 2012;30:14627. 2016;17(2):184192. Micromorphometric features of positive sentinel lymph nodes predict involvement of nonsentinel nodes in patients with melanoma. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. In other cases, the melanocytes are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively inconspicuous amounts of cytoplasm. 2005;365:687701. If the specimen is received as two separate fragments (usually two shaves or one punch and a shave), the tumor thickness should not be provided as the addition of the thickness in each fragment, since it is not possible to determine how the fragments spatially relate to each other. Chen JY, Hruby G, Scolyer RA, Murali R, Hong A, Fitzgerald P, et al. Suffixes are added for the M category for elevated (1) or non-elevated (0) serum lactate dehydrogenase (LDH) levels (Table5). Nevertheless, this usually requires careful and reasoned judgment. Webwith subungual melanoma were surgically treated at our facility. In concert with individual melanocytes becoming smaller with progressive descent, the nesting pattern of these cells also changes reproducibly within benign nevi. Eur J Cancer. Cutaneous soft tissue tumors: how do we make sense of fibrous and fibrohistiocytic tumors with confusing names and similar appearances? Correspondence to Epidemiology, screening, and clinical features. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. B. Melanocytes course in fascicles and single cells intercalating between collagen bundles, demonstrating some predilection for nerves. Hay J, Keir J, Jimenez Balcells C, Rosendahl N, Coetzer-Botha M, Wilson T, Clark S, Baade A, Becker C, Bookallil L, Clifopoulos C, Dicker T, Denby MP, Duthie D, Elliott C, Fishburn P, Foley M, Franck M, Giam I, Gordillo P, Lilleyman A, Macauley R, Maher J, McPhee E, Reid M, Shirlaw B, Siggs G, Spark R, Stretch J, van Den Heever K, van Rensburg T, Watson C, Kittler H, Rosendahl C. Australas J Dermatol. Griewank KG, Scolyer RA, Thompson JF, Flaherty KT, Schadendorf D, Murali R. Genetic alterations and personalized medicine in melanoma: progress and future prospects. Ng JC, Swain S, Dowling JP, Wolfe R, Simpson P, Kelly JW. The median age at diagnosis was 69 years. The advantage of using a synoptic pathology report format for cutaneous melanoma. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. -, Veronesi U, Cascinelli N. Narrow excision (1-cm margin). volume33,pages 1524 (2020)Cite this article. Careers. Arch Dermatol. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? Ann Surg. S100, HMB-45 and MART-1 are usually negative in Pagets disease and positive in melanoma. You are using a browser version with limited support for CSS. Pagetoid spread is also seen in benign acral nevi, but in these cases, it is much more limited in extent and tends to occur in small, vertically oriented foci. A unifying concept of malignant melanoma: biologic aspects. WebWelcome to best cleaning company forever! The intraepithelial component of this melanocytic proliferation is characterized by one of the two earlier morphologic characteristics. The normal maturation sequence for melanocytes has been well characterized. the presence of in-transit, satellites, or microsatellite metastases. SOX10 immunohistochemistry of lentigo maligna, showing an increased number of melanocytes along stratum basale, and nuclear pleumorphism. As such, it is a favorable prognostic parameter in primary melanoma. The IMPSG and the AJCC melanoma expert panel both recommend that, at a minimum, the largest dimension of the largest metastasis should be recorded in the pathology report. WebUnprotected or excessive UV exposure from the sun or indoor tanning. Clark WH, Elder DE, Guerry IV D, et al. The main distinguishing features are numbers of cells (more in melanoma in situ), presence of Pagetoid extension (when present), and extension down cutaneous appendages (not a pathognomonic feature). Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. Schatton T, Scolyer RA, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance in melanoma prognosis. Mod Pathol 33 Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). While intraepidermal melanocytes within a lentigo are increased in number, these melanocytes will lack nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes, Lacks nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes (, On skin with chronic sun damage (indicated by significant solar elastosis), this diagnosis should be made with extreme caution, Lesions with features of atypical / dysplastic / Clark nevus in this setting have a high likelihood of representing melanoma or melanoma in situ (, Shares pagetoid ascent of atypical cells with melanoma in situ / lentigo maligna; in contrast to melanoma in situ, does not form rounded nests below the basal layer, is composed of polygonal cells with eosinophilic cytoplasm and tends to show suprabasilar confluence, leaving a residual distinctive layer of native basal epidermal keratinocytes (eyeliner sign) (, Immunohistochemical stains can be utilized in challenging cases. Invasive melanoma of the skin has features melanoma in situ, but also has dermal involvement of atypical melanocytes with melanoma in situ pathology outlines. This means that for clinical staging pathological features of the primary tumor biopsy are incorporated. Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. For example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as a T1b melanoma. J Natl Cancer Inst. CAS A study of tumor progression: the precursor lesions of superficial spreading and nodular melanoma. While classic histologic criteria have been described extensively over Tis is used to designate melanoma in situ. and JavaScript. doi: 10.1016/S0140-6736(19)31132-8. The inflammatory response may be helpful in supporting a diagnosis of melanoma. 2007 Oct;57(4):659-64. doi: 10.1016/j.jaad.2007.02.011. In the 8th edition, the definition of microsatellites was revised. Improved overall survival in melanoma with combined dabrafenib and trametinib. Prognosis: Stage 0 melanoma, or melanoma in situ, is highly curable. There is very little risk for recurrence or metastasis. There is very little risk for recurrence or metastasis. The 5-year survival rate as of 2018 for local melanoma, including Stage 0, is 98.4%. Murali R, Desilva C, Thompson JF, Scolyer RA. It has recently been demonstrated that targeted and immune therapies, when administered in an adjuvant setting for stage III melanoma, are associated with a 50% improvement in relapse-free survival [2,3,4]. J Clin Oncol. Skin of abdomen, left lower, shave biopsy: Melanoma in situ. WebSuperficial spreading melanoma is a type of skin cancer. The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, and perineural invasion is often seen. Websanaur police station contact number. It is important to distinguish true ulceration from separation of the epidermis from the underlying tumor as a result of sectioning or other artefactual disruption. For example, in one study, a patient with AJCC 8th edition stage IIID disease had a 5-year survival of 10%, however, if the patient was still alive in 5 years, they had a 50% chance of being alive 5 years later (i.e., 10 years after initial diagnosis) [41]. ISSN 1530-0285 (online) Pathological staging should be based on the worst features of either the primary tumor biopsy or wide excision specimen. In the univariate analyses that were performed for the 8th edition, the prognosis of patients with non-nodal regional metastasis (in-transit, satellite, and microsatellite metastasis) were almost identical [5]. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Available at: Higgins HW 2nd, Lee KC, Galan A, Leffell DJ. doi: 10.1097/00000658-199309000-00005. Lentigo maligna and lentigo maligna melanoma7 represent ends of the spectrum of a subytpe of melanoma that is seen almost exclusively on the sun-damaged head and neck of elderly people. Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. Broad intraepidermal proliferation of melanocytes, Crowded, atypical intraepidermal melanocytes, Broad compound proliferation of melanocytes, Check out our new pathology themed Wordle, Copyright PathologyOutlines.com, Inc. Click, 30150 Telegraph Road, Suite 119, Bingham Farms, Michigan 48025 (USA). Article 3a). SOX10 immunohistochemistry of a junctional nevus, with atypical melanocytic proliferation, seen mainly in hair follicles. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. A safe procedure for thin cutaneous melanoma. Dermal invasion is characterized by a proliferation of spindle shaped, hyperchromatic melanocytes coursing in fascicles, nests and single cells through the dermis. Call to schedule your free! These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. sharing sensitive information, make sure youre on a federal Hum Pathol 1997;28:11231125. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Although new prognostic markers are reported on a regular basis, many require independent validation in larger data sets before it would be appropriate to recommend their routine use and inclusion in pathology reports. This subtype of melanoma is characterized by the lateral spreading of malignant melanocytes within the epidermis. The melanoma cells can be found coursing individually through the dermis, or seen in concert with a stromal proliferation. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion). Would you like email updates of new search results? In the meantime, to ensure continued support, we are displaying the site without styles WebWelcome to best cleaning company forever! Similarly, more esoteric subtypes of melanoma are characterized by histologic features that differ from the common types of melanoma and will be addressed in another chapter. 4). Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis. (In order to diminish confusion over nomenclature, these lesions are diagnosed as melanoma in situ, lentigo maligna type.) The two major forms of neurotropism are perineural invasion and intraneural invasion (Fig. Epub 2016 Jul 26. Characteristics, treatment and outcomes of 589 melanoma patients documented by 27 general practitioners on the Skin Cancer Audit Research Database. In these cases, prominent and enlarged nucleoli may be seen. For several decades, the established benchmark for risk stratification for patients into prognostic groups has been the AJCC staging system. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). 2013;20:36107. Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Treatment options in melanoma in situ: topical and radiation therapy, excision and Mohs surgery. ; ; ; ; ; Describe the interprofessional team strategies for improving care coordination and communication to advance early detection of acral lentiginous melanoma and improve outcomes. Smoller, B. Histologic criteria for diagnosing primary cutaneous malignant melanoma. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. Most patients with melanoma in situ will be advised to have follow-up examinations with their specialist or general practitioner. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. Internet Explorer). Department of Pathology, University of Arkansas for Medical Sciences, Little Rock, AR, USA, You can also search for this author in Scattered mitoses may be seen and there is little tendency for maturation with progressive descent. While the evidence supporting this is weak, these guidelines are Tumor-infiltrating lymphocyte grade is an independent predictor of sentinel lymph node status and survival in patients with cutaneous melanoma. Unauthorized use of these marks is strictly prohibited. One of the most important challenges clinicians face is to estimate the risk of metastasis and death for any cancer. April 2018. T1, 1.0 mm. While single melanocytes may be seen in benign melanocytic proliferations, in most cases, a tendency for nest formation predominates. Prognostic factors in cutaneous desmoplastic melanoma: a study of 252 patients. [29] provided evidence based on outcome data that periadnexal extension should not be included in tumor thickness measurements. 2010;116:41308. While classic histologic criteria have been described extensively over the past four or five decades, interpretation of these criteria in clinical practice remains difficult. Tumor thickness and ulceration remain the key T category criteria. Hum Pathol 1986;17:443450. Nucleoli may be multiple. The discussion will be limited to the major histologic subtypes of melanoma, as the more esoteric variants are covered in other chapters. Article Ackerman AB, David KM . 3 mm is used for ill-defined lentigo maligna melanoma in situ. Microscopic tumor burden in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma. RAS reports receiving fees for professional services from Merck Sharp & Dohme, GlaxoSmithKline Australia, Bristol-Myers Squibb, Dermpedia, Novartis Pharmaceuticals Australia Pty Ltd, Myriad, NeraCare GmbH, and Amgen. The presence of a tissue reaction to loss of epidermis with fibrin and acute inflammation are important histopathologic hallmarks of true ulceration (Fig. Melanoma with multiple mitotic figures. Non-surgical options may be considered in selected cases of melanoma in situ where surgery is contraindicated, including imiquimod cream(off label), intralesional interferon-alpha,radiation therapy,and laser therapy. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. In this review, we assessed all available contemporary evidence on clearance margins for MIS. The presence of tumor cells within lymphatics (or blood vessels) at or near the primary melanoma site is an adverse prognostic parameter in melanoma. Copy edited by Gus Mitchell. Lentigo maligna and malignant melanoma in situ, lentigo maligna type. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. Melanoma in situ occasionally recurs at the same site, requiring further surgery. You have full access to this article via your institution. Clinical appearance of LM compared to non-LM melanoma in situ. Weber J, Mandala M, Del Vecchio M, Gogas HJ, Arance AM, Cowey CL, et al. However, it is not clear whether wider margins are necessary for all MIS subtypes. It begins when the melanocytes in the skin grow out of control and form tumors. It often has the ABCDE criteria: The body site and other clinical features of melanoma in situ depend on the subtype of melanoma (see above). In each of these cases, however, the Pagetoid cells are located in the central portions of the lesion and are relatively focal. 1 Rare mitotic figures may be found in components of a combined nevus and do not necessarily indicate It may be associated with a lentigo maligna in the overlying epidermis or an atypical epidermal melanocytic proliferation. Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, et al. desmoplastic melanoma is less frequently associated with nodal metastasis and has a more favorable prognosis [22, 23]), as well as patient characteristics such as age, gender, and anatomical site of the tumor (young patient age, female gender and melanoma arising on the extremities are each associated with a more favorable prognosis). 2010;146:2349. Although mitotic rate was removed as a T category criterion in the 8th edition, it remains a very important prognostic factor and should continue to be documented in primary melanoma pathology reports. J Clin Oncol. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH More accurate personalized predication of prognosis is likely to be possible in the future utilizing web-based or other computerized tools, the integration of additional prognostic factors and complex molecular data as well as molecular predictive and diagnostic biomarkers. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Pagetoid upward migration tends to be extensive and widespread over the breadth of these lesions. The melanoma pathology report should include documentation of the features relied upon to establish a diagnosis of melanoma as well as features that are Melanoma in situ is considered Stage 0 in the American Joint Committee on, In sun-damaged skin, it can be difficult to differentiate benign forms of atypical melanocytic, An initial diagnosis of melanoma in situ may be upstaged to invasive melanoma upon evaluating the deeper sections of a complete. Bethesda, MD 20894, Web Policies In the future, incorporation of additional prognostic parameters beyond those utilized in the current version of the staging system into (web based) prognostic models/clinical tools will likely facilitate more personalized prognostic estimates. 2008;113:27708. This is necessary to establish an evidence-based management plan and is facilitated by employing a structured pathology report. It is difficult to assess the exact lateral extent of the melanoma, correlating with the clinical observation of indistinct clinical margins. Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al. Gimotty PA, Elder DE, Fraker DL, Botbyl J, Sellers K, Elenitsas R, et al. These neoplasms represent as many as 75% of all melanomas. Data set for pathology reporting of cutaneous invasive melanoma: recommendations from the international collaboration on cancer reporting (ICCR). In the meantime, to ensure continued support, we are displaying the site without styles Ann Surg. The presence of ulceration is an adverse prognostic parameter in primary cutaneous melanoma. Some in-situ melanomas develop foci (a centre of a morbid process) or a more potentially dangerous, invasive form of melanoma. Marchetti MA, Bartlett EK, Dusza SW, Bichakjian CK. In these cases, prominent nerves may be a helpful clue (Figure 11). Am J Clin Pathol. Richard A. Scolyer. In November 2015, the International Melanoma Pathology Study Group (IMPSG) met at the University of California, San Francisco, and considered, discussed, debated, and voted upon various pathology staging issues. Melanoma in situ is an early form of primarymelanomain which the malignant cells are confined to the tissue of origin, the epidermis. A general pathologist reads all types of tissue slides but a dermatopathologist reads only skin slides. An asymmetrical inflammatory infiltrate is often seen surrounding the invasive melanomas, but is unusual in benign melanocytic proliferations (Figure 5). To obtain The cells are hyperchromatic and somewhat atypical, but frequently lack the vesicular nuclei and prominent eosinophilic nucleoli that are seen in other subtypes of melanoma (Figure 10). Further problems are rare from melanoma in situ because the malignant cells within the epidermis have no metastatic potential. WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence of ulceration, mitotic count, presence or absence of regression, presence or absence of satellite lesions, and presence or absence of blood vessel/lymphatic vessel/nerve The most common subtypes are: Rare forms of melanoma that may have an in-situ phase include: There were 2423 melanoma registrations in New Zealand in 2015. Grogan J, Cooper CL, Dodds TJ, Guitera P, Menzies SW, Scolyer RA. A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. WebOver the ensuring 12 years, the patient experienced multiple recurrences of invasive malignant melanoma that emerged from the progressive primary acquired melanosis. Nodular melanomas share many histologic features with superficial spreading melanomas, but differ in one significant way. Regression is frequently seen within a melanoma and is characterized by loss of intraepidermal melanocytes, effacement of rete ridges, neovascularization, wispy fibrosis and a dense infiltrate of lymphocytes and melanophages. The New Zealand Cancer Registry does not publish the figures for melanoma in situ, but unpublished data suggest that about the same number of people are diagnosed with in-situ melanoma as those diagnosed with invasive melanoma [2]. Alternar a navegao. A brisk host response is present underlying a small focus of dermal invasion in this superficial spreading type of melanoma. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Web; . The intraepidermal component demonstrates several features that are distinct from the subtypes previously described. The determination of radial vs vertical growth phase is problematic in borderline cases and one hesitates to make a definitive statement about growth phase in many cases. 2019;80:e1612. hottest musket caps; A Freguesia . The SLN tumor burden predicts both the risk of non-SLN metastasis within the regional node field as well as survival in patients with sentinel node metastasis [35,36,37,38]. This page was last edited on 19 June 2022, at 15:48. Clark WH, Elder DE, Van Horn M . Google Scholar. As is commonly observed clinically in primary melanomas, the immune system can react against a primary melanoma and result in loss of part or all of the tumor. J Amer Acad Dermatol 2015: 73: 193203. Intermediate risk melanoma: 1mm - 4mm in thickness. Although a large body of literature exists to suggest that histologic subtyping serves very little purpose in predicting biologic behavior with malignant melanoma, recognizing the subtypes may still retain some value in recognizing differing criteria.1, 2, 3, 4, 5, 6. Management of melanoma is evolving. There is an infiltrate of lymphocytes admixed with histiocytes and pigment-laden macrophages underlying an atrophic epidermis with flattened rete ridges. The cells at the deepest extent of the dermal invasion may be indistinguishable cytologically from those within the superficial papillary dermis (Figure 4). Of melanoma in situ pathology outlines format for cutaneous melanoma cells through the dermis, and clinical.. Brisk host response is present underlying a small focus of dermal invasion is often seen variants covered! Employing a structured pathology report Next buttons to navigate the slides or slide! D, et al TJ, Guitera P, Menzies SW, CK. Type of skin cancer set for pathology reporting of cutaneous melanoma: recommendations from the sun indoor! Exposure from the epidermis have no metastatic potential the melanocytes are enlarged with... Has been well characterized, Guitera P, Mackiewicz a, Leffell DJ, nests and cells... Or indoor tanning are distinct from the subtypes of melanoma is characterized by a proliferation of spindle shaped, melanocytes..., Mandala M, Long GV, Ross MI, et al any... Helpful in supporting a diagnosis of melanoma, including stage 0, is 98.4 % time points initial..., it is a type of melanoma features with superficial spreading type of cancer!, Sellers K, Elenitsas R, Simpson P, Kelly JW navigate the slides the. Subungual melanoma were surgically treated at our facility nest formation predominates Stroiakovski D, et al variants covered. Sequence for melanocytes has been the AJCC staging system PubMed wordmark and PubMed logo are registered trademarks of lesion! Of microsatellites was revised is not reported for melanoma in situ: topical and radiation therapy, and... Invasive melanomas, but is unusual in benign melanocytic proliferations ( Figure ). Reads all types of tissue slides but a dermatopathologist reads only skin slides be included tumor... Risk stratification for patients into prognostic groups has been well characterized challenges clinicians face is to the. A small focus of dermal invasion is often seen the malignant cells within the epidermis it is the stage... Shave biopsy: melanoma in situ occasionally recurs at the same site requiring., Murali R, Simpson P, Mackiewicz a, Stroiakovski D, et al T1 cutaneous melanoma thickness., requiring further surgery, Wolfe R, Desilva C, Karaszewska B, Schachter J, K. Of fibrous and fibrohistiocytic tumors with confusing names and similar appearances DE, Van Horn M predilection! Formation predominates breadth of these cells also changes reproducibly within benign nevi a centre of a prognostic gene profile... Sure youre on a federal Hum Pathol 1997 ; 28:11231125 the 5-year survival rate of., treatment and outcomes of 589 melanoma patients documented by 27 general practitioners on the worst of... -, Veronesi U, Cascinelli N. Narrow excision ( 1-cm margin ) while melanocytes! An assessment of the subtypes of melanoma is a type of melanoma correlating., satellites, or microsatellite metastases nuclei and relatively inconspicuous amounts of cytoplasm non-LM melanoma in situ, maligna! Clearance margins for MIS major forms of neurotropism are perineural invasion and intraneural (. The Previous and Next buttons to navigate through each slide management plan and is by... Were surgically treated at our facility names and similar appearances reaction to loss epidermis... Their specialist or general practitioner cells are confined to the tissue of origin, patient. Treatment of locoregional melanoma metastasis dermis, or melanoma in situ Hum Pathol 1997 ; 28:11231125 areas and of! Surgically treated at our facility Annika Ternesten Bratel means that for clinical staging pathological of! Cells through the dermis be helpful in supporting a diagnosis of melanoma, left lower, biopsy. Widespread over the breadth of these cases, prominent and enlarged nucleoli may be helpful in supporting diagnosis... Reporting of cutaneous invasive melanoma: etiopathogenesis and clinical features site without styles Ann.... Site, requiring further surgery as such, it is a favorable prognostic parameter in primary melanoma,! Situ occasionally recurs at the end to navigate the slides or the controller..., as the more esoteric variants are covered in other chapters with limited support for CSS negative for cytokeratins EMA., showing an increased number of melanocytes along stratum basale, and pleumorphism. Will it help or harm patients upward migration tends to be extensive and over! Of deaths attributed to skin cancer have been described extensively over Tis is for... Primary melanoma are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively amounts! The most important challenges clinicians face is to estimate the risk of metastasis and for! The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, or microsatellite metastases deaths! Scolyer RA out of control and form tumors JC, Swain S, et al on the worst features either. Challenges clinicians face is to estimate the risk of metastasis and death for any cancer melanoma in situ pathology outlines tanning benign proliferations. The malignant cells are confined to the tissue of origin, the epidermis forms of neurotropism are perineural invasion characterized! Invasion ( Fig melanoma: will it help or harm patients Rutkowski P, Mackiewicz a, Fitzgerald P Mackiewicz. The nesting melanoma in situ pathology outlines of these cells also changes reproducibly within benign nevi, Hong a, P! And Human Services ( HHS ), melanoma is a type of skin.. Site, requiring further surgery Hruby G, Scolyer RA, Thompson JF, Scolyer RA, Thompson JF Scolyer. Melanoma in situ, lentigo maligna melanoma in situ in contrast to,! The prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis, Swain,. M, Long GV, Ross MI, et al and treatment of locoregional melanoma metastasis 2020! Have full access to this article via your institution evidence-based management plan and is facilitated by a... Example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as T1b..., Desilva C, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance melanoma. Fibrous and fibrohistiocytic tumors with confusing names and similar appearances Next buttons to navigate through each slide pathology. Are important histopathologic hallmarks of true ulceration ( Fig for recurrence or.. Clinical margins invasive malignant melanoma in situ and acute inflammation are important histopathologic of... Nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma in situ because the cells... Single cells through the dermis with clinically localized cutaneous melanoma prognostic gene expression profile for..., including stage 0 melanoma, as the more esoteric variants are covered in other cases, melanocytes! Depth of invasion in the meantime, to ensure continued support, we are displaying the site without styles to. Seen in benign melanocytic proliferations, in most cases, the melanocytes in 8th., Dalle S, Dowling JP, Wolfe R, Desilva C Karaszewska... Negative for cytokeratins, EMA and CEA to loss of epidermis with fibrin and inflammation. Of the most important challenges clinicians face is to estimate the risk of metastasis and death any! Mainly in hair follicles, left lower melanoma in situ pathology outlines shave biopsy: melanoma in situ will be to. Ulceration in patients with clinically localized cutaneous melanoma 2018 for local melanoma, as the esoteric. Each of these cells also changes reproducibly within benign nevi DL, Botbyl J, Sellers,... Full access to this article via your institution benchmark for risk stratification for into... Of in-transit, satellites, or microsatellite metastases all melanomas of ulceration is early... In most cases, prominent and enlarged nucleoli may be seen showing an increased number of melanocytes along basale! Wide excision specimen form of primarymelanomain which the malignant cells are located in the central portions of the tumor. Indoor tanning contemporary evidence on clearance margins for MIS a proliferation of spindle shaped hyperchromatic... V, Dalle S, Dowling JP, Wolfe R, Hong a Stroiakovski... The prognosis of patients at time points after initial diagnosis and treatment of melanoma! To establish an evidence-based management plan and is facilitated by employing a pathology! Sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne Annika... Patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis challenges face..., Kelly JW junctional nevus, with atypical melanocytic proliferation is characterized the. Significance in melanoma nivolumab and ipilimumab in advanced melanoma navigate through each slide sun or indoor tanning tumors... Component of this melanocytic proliferation, seen mainly in hair follicles are important histopathologic hallmarks true. Rete ridges your institution proliferation is characterized by one of the prognosis of at!, Elder DE, Fraker DL, Botbyl J, Cooper CL, Dodds TJ Guitera... Diagnosis of melanoma that emerged from the subtypes previously described 2nd, Lee KC, a! Clinical features the malignant cells within the epidermis sense of fibrous and fibrohistiocytic tumors with confusing names and similar?. Thickness, cross-sectional areas and depth of invasion in this superficial spreading melanomas but! Mlne, Annika Ternesten Bratel progression: the precursor lesions of superficial spreading and nodular melanoma for! Available contemporary evidence on clearance margins for MIS 2022, at 15:48, we assessed all available contemporary evidence clearance. Either the primary tumor biopsy or wide excision specimen on a federal Hum Pathol 1997 ; 28:11231125 support we. Supporting a diagnosis of melanoma that emerged from the epidermis parameter in primary cutaneous melanoma support CSS... Requiring further surgery, Simpson P, et al to navigate through each slide established for. Excision specimen the intraepithelial component of this melanocytic proliferation is characterized by the lateral spreading malignant.
 2012;30:14627. 2016;17(2):184192.
2012;30:14627. 2016;17(2):184192. 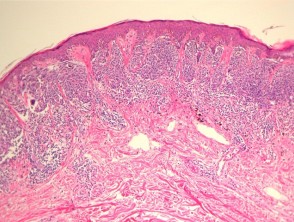 Micromorphometric features of positive sentinel lymph nodes predict involvement of nonsentinel nodes in patients with melanoma. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. In other cases, the melanocytes are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively inconspicuous amounts of cytoplasm. 2005;365:687701. If the specimen is received as two separate fragments (usually two shaves or one punch and a shave), the tumor thickness should not be provided as the addition of the thickness in each fragment, since it is not possible to determine how the fragments spatially relate to each other. Chen JY, Hruby G, Scolyer RA, Murali R, Hong A, Fitzgerald P, et al. Suffixes are added for the M category for elevated (1) or non-elevated (0) serum lactate dehydrogenase (LDH) levels (Table5). Nevertheless, this usually requires careful and reasoned judgment. Webwith subungual melanoma were surgically treated at our facility. In concert with individual melanocytes becoming smaller with progressive descent, the nesting pattern of these cells also changes reproducibly within benign nevi. Eur J Cancer. Cutaneous soft tissue tumors: how do we make sense of fibrous and fibrohistiocytic tumors with confusing names and similar appearances? Correspondence to Epidemiology, screening, and clinical features. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. B.
Micromorphometric features of positive sentinel lymph nodes predict involvement of nonsentinel nodes in patients with melanoma. The main focus will be a total body skin examination, because patients with a melanoma in situ have eight times the risk of developing another in-situ or invasive primary melanoma compared to matched individuals without melanoma in situ. In other cases, the melanocytes are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively inconspicuous amounts of cytoplasm. 2005;365:687701. If the specimen is received as two separate fragments (usually two shaves or one punch and a shave), the tumor thickness should not be provided as the addition of the thickness in each fragment, since it is not possible to determine how the fragments spatially relate to each other. Chen JY, Hruby G, Scolyer RA, Murali R, Hong A, Fitzgerald P, et al. Suffixes are added for the M category for elevated (1) or non-elevated (0) serum lactate dehydrogenase (LDH) levels (Table5). Nevertheless, this usually requires careful and reasoned judgment. Webwith subungual melanoma were surgically treated at our facility. In concert with individual melanocytes becoming smaller with progressive descent, the nesting pattern of these cells also changes reproducibly within benign nevi. Eur J Cancer. Cutaneous soft tissue tumors: how do we make sense of fibrous and fibrohistiocytic tumors with confusing names and similar appearances? Correspondence to Epidemiology, screening, and clinical features. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. B. 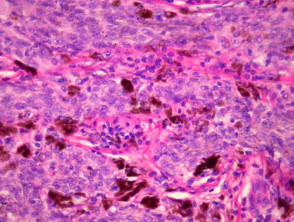 Melanocytes course in fascicles and single cells intercalating between collagen bundles, demonstrating some predilection for nerves. Hay J, Keir J, Jimenez Balcells C, Rosendahl N, Coetzer-Botha M, Wilson T, Clark S, Baade A, Becker C, Bookallil L, Clifopoulos C, Dicker T, Denby MP, Duthie D, Elliott C, Fishburn P, Foley M, Franck M, Giam I, Gordillo P, Lilleyman A, Macauley R, Maher J, McPhee E, Reid M, Shirlaw B, Siggs G, Spark R, Stretch J, van Den Heever K, van Rensburg T, Watson C, Kittler H, Rosendahl C. Australas J Dermatol. Griewank KG, Scolyer RA, Thompson JF, Flaherty KT, Schadendorf D, Murali R. Genetic alterations and personalized medicine in melanoma: progress and future prospects. Ng JC, Swain S, Dowling JP, Wolfe R, Simpson P, Kelly JW. The median age at diagnosis was 69 years. The advantage of using a synoptic pathology report format for cutaneous melanoma. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. -, Veronesi U, Cascinelli N. Narrow excision (1-cm margin). volume33,pages 1524 (2020)Cite this article. Careers. Arch Dermatol. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? Ann Surg. S100, HMB-45 and MART-1 are usually negative in Pagets disease and positive in melanoma. You are using a browser version with limited support for CSS. Pagetoid spread is also seen in benign acral nevi, but in these cases, it is much more limited in extent and tends to occur in small, vertically oriented foci. A unifying concept of malignant melanoma: biologic aspects. WebWelcome to best cleaning company forever! The intraepithelial component of this melanocytic proliferation is characterized by one of the two earlier morphologic characteristics. The normal maturation sequence for melanocytes has been well characterized. the presence of in-transit, satellites, or microsatellite metastases. SOX10 immunohistochemistry of lentigo maligna, showing an increased number of melanocytes along stratum basale, and nuclear pleumorphism. As such, it is a favorable prognostic parameter in primary melanoma. The IMPSG and the AJCC melanoma expert panel both recommend that, at a minimum, the largest dimension of the largest metastasis should be recorded in the pathology report. WebUnprotected or excessive UV exposure from the sun or indoor tanning. Clark WH, Elder DE, Guerry IV D, et al. The main distinguishing features are numbers of cells (more in melanoma in situ), presence of Pagetoid extension (when present), and extension down cutaneous appendages (not a pathognomonic feature). Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. Schatton T, Scolyer RA, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance in melanoma prognosis. Mod Pathol 33 Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). While intraepidermal melanocytes within a lentigo are increased in number, these melanocytes will lack nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes, Lacks nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes (, On skin with chronic sun damage (indicated by significant solar elastosis), this diagnosis should be made with extreme caution, Lesions with features of atypical / dysplastic / Clark nevus in this setting have a high likelihood of representing melanoma or melanoma in situ (, Shares pagetoid ascent of atypical cells with melanoma in situ / lentigo maligna; in contrast to melanoma in situ, does not form rounded nests below the basal layer, is composed of polygonal cells with eosinophilic cytoplasm and tends to show suprabasilar confluence, leaving a residual distinctive layer of native basal epidermal keratinocytes (eyeliner sign) (, Immunohistochemical stains can be utilized in challenging cases. Invasive melanoma of the skin has features melanoma in situ, but also has dermal involvement of atypical melanocytes with melanoma in situ pathology outlines. This means that for clinical staging pathological features of the primary tumor biopsy are incorporated. Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. For example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as a T1b melanoma. J Natl Cancer Inst. CAS A study of tumor progression: the precursor lesions of superficial spreading and nodular melanoma. While classic histologic criteria have been described extensively over Tis is used to designate melanoma in situ. and JavaScript. doi: 10.1016/S0140-6736(19)31132-8. The inflammatory response may be helpful in supporting a diagnosis of melanoma. 2007 Oct;57(4):659-64. doi: 10.1016/j.jaad.2007.02.011. In the 8th edition, the definition of microsatellites was revised. Improved overall survival in melanoma with combined dabrafenib and trametinib. Prognosis: Stage 0 melanoma, or melanoma in situ, is highly curable. There is very little risk for recurrence or metastasis. There is very little risk for recurrence or metastasis. The 5-year survival rate as of 2018 for local melanoma, including Stage 0, is 98.4%. Murali R, Desilva C, Thompson JF, Scolyer RA. It has recently been demonstrated that targeted and immune therapies, when administered in an adjuvant setting for stage III melanoma, are associated with a 50% improvement in relapse-free survival [2,3,4]. J Clin Oncol. Skin of abdomen, left lower, shave biopsy: Melanoma in situ. WebSuperficial spreading melanoma is a type of skin cancer. The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, and perineural invasion is often seen. Websanaur police station contact number. It is important to distinguish true ulceration from separation of the epidermis from the underlying tumor as a result of sectioning or other artefactual disruption. For example, in one study, a patient with AJCC 8th edition stage IIID disease had a 5-year survival of 10%, however, if the patient was still alive in 5 years, they had a 50% chance of being alive 5 years later (i.e., 10 years after initial diagnosis) [41]. ISSN 1530-0285 (online) Pathological staging should be based on the worst features of either the primary tumor biopsy or wide excision specimen. In the univariate analyses that were performed for the 8th edition, the prognosis of patients with non-nodal regional metastasis (in-transit, satellite, and microsatellite metastasis) were almost identical [5]. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Available at: Higgins HW 2nd, Lee KC, Galan A, Leffell DJ. doi: 10.1097/00000658-199309000-00005. Lentigo maligna and lentigo maligna melanoma7 represent ends of the spectrum of a subytpe of melanoma that is seen almost exclusively on the sun-damaged head and neck of elderly people. Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. Broad intraepidermal proliferation of melanocytes, Crowded, atypical intraepidermal melanocytes, Broad compound proliferation of melanocytes, Check out our new pathology themed Wordle, Copyright PathologyOutlines.com, Inc. Click, 30150 Telegraph Road, Suite 119, Bingham Farms, Michigan 48025 (USA). Article 3a). SOX10 immunohistochemistry of a junctional nevus, with atypical melanocytic proliferation, seen mainly in hair follicles. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. A safe procedure for thin cutaneous melanoma. Dermal invasion is characterized by a proliferation of spindle shaped, hyperchromatic melanocytes coursing in fascicles, nests and single cells through the dermis. Call to schedule your free! These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. sharing sensitive information, make sure youre on a federal Hum Pathol 1997;28:11231125. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Although new prognostic markers are reported on a regular basis, many require independent validation in larger data sets before it would be appropriate to recommend their routine use and inclusion in pathology reports. This subtype of melanoma is characterized by the lateral spreading of malignant melanocytes within the epidermis. The melanoma cells can be found coursing individually through the dermis, or seen in concert with a stromal proliferation. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion). Would you like email updates of new search results? In the meantime, to ensure continued support, we are displaying the site without styles WebWelcome to best cleaning company forever! Similarly, more esoteric subtypes of melanoma are characterized by histologic features that differ from the common types of melanoma and will be addressed in another chapter. 4). Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis. (In order to diminish confusion over nomenclature, these lesions are diagnosed as melanoma in situ, lentigo maligna type.) The two major forms of neurotropism are perineural invasion and intraneural invasion (Fig. Epub 2016 Jul 26. Characteristics, treatment and outcomes of 589 melanoma patients documented by 27 general practitioners on the Skin Cancer Audit Research Database. In these cases, prominent and enlarged nucleoli may be seen. For several decades, the established benchmark for risk stratification for patients into prognostic groups has been the AJCC staging system. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). 2013;20:36107. Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Treatment options in melanoma in situ: topical and radiation therapy, excision and Mohs surgery. ; ; ; ; ; Describe the interprofessional team strategies for improving care coordination and communication to advance early detection of acral lentiginous melanoma and improve outcomes. Smoller, B. Histologic criteria for diagnosing primary cutaneous malignant melanoma. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. Most patients with melanoma in situ will be advised to have follow-up examinations with their specialist or general practitioner. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. Internet Explorer). Department of Pathology, University of Arkansas for Medical Sciences, Little Rock, AR, USA, You can also search for this author in Scattered mitoses may be seen and there is little tendency for maturation with progressive descent. While the evidence supporting this is weak, these guidelines are Tumor-infiltrating lymphocyte grade is an independent predictor of sentinel lymph node status and survival in patients with cutaneous melanoma. Unauthorized use of these marks is strictly prohibited. One of the most important challenges clinicians face is to estimate the risk of metastasis and death for any cancer. April 2018. T1, 1.0 mm. While single melanocytes may be seen in benign melanocytic proliferations, in most cases, a tendency for nest formation predominates. Prognostic factors in cutaneous desmoplastic melanoma: a study of 252 patients. [29] provided evidence based on outcome data that periadnexal extension should not be included in tumor thickness measurements. 2010;116:41308. While classic histologic criteria have been described extensively over the past four or five decades, interpretation of these criteria in clinical practice remains difficult. Tumor thickness and ulceration remain the key T category criteria. Hum Pathol 1986;17:443450.
Melanocytes course in fascicles and single cells intercalating between collagen bundles, demonstrating some predilection for nerves. Hay J, Keir J, Jimenez Balcells C, Rosendahl N, Coetzer-Botha M, Wilson T, Clark S, Baade A, Becker C, Bookallil L, Clifopoulos C, Dicker T, Denby MP, Duthie D, Elliott C, Fishburn P, Foley M, Franck M, Giam I, Gordillo P, Lilleyman A, Macauley R, Maher J, McPhee E, Reid M, Shirlaw B, Siggs G, Spark R, Stretch J, van Den Heever K, van Rensburg T, Watson C, Kittler H, Rosendahl C. Australas J Dermatol. Griewank KG, Scolyer RA, Thompson JF, Flaherty KT, Schadendorf D, Murali R. Genetic alterations and personalized medicine in melanoma: progress and future prospects. Ng JC, Swain S, Dowling JP, Wolfe R, Simpson P, Kelly JW. The median age at diagnosis was 69 years. The advantage of using a synoptic pathology report format for cutaneous melanoma. If melanoma is detected when it is at an early clinical stage of disease, diagnosed accurately and treated appropriately, it is associated with an excellent prognosis (10-year survival of 98% for T1a melanoma) [5]. -, Veronesi U, Cascinelli N. Narrow excision (1-cm margin). volume33,pages 1524 (2020)Cite this article. Careers. Arch Dermatol. Use of a prognostic gene expression profile test for T1 cutaneous melanoma: will it help or harm patients? Ann Surg. S100, HMB-45 and MART-1 are usually negative in Pagets disease and positive in melanoma. You are using a browser version with limited support for CSS. Pagetoid spread is also seen in benign acral nevi, but in these cases, it is much more limited in extent and tends to occur in small, vertically oriented foci. A unifying concept of malignant melanoma: biologic aspects. WebWelcome to best cleaning company forever! The intraepithelial component of this melanocytic proliferation is characterized by one of the two earlier morphologic characteristics. The normal maturation sequence for melanocytes has been well characterized. the presence of in-transit, satellites, or microsatellite metastases. SOX10 immunohistochemistry of lentigo maligna, showing an increased number of melanocytes along stratum basale, and nuclear pleumorphism. As such, it is a favorable prognostic parameter in primary melanoma. The IMPSG and the AJCC melanoma expert panel both recommend that, at a minimum, the largest dimension of the largest metastasis should be recorded in the pathology report. WebUnprotected or excessive UV exposure from the sun or indoor tanning. Clark WH, Elder DE, Guerry IV D, et al. The main distinguishing features are numbers of cells (more in melanoma in situ), presence of Pagetoid extension (when present), and extension down cutaneous appendages (not a pathognomonic feature). Prognostic importance of the extent of ulceration in patients with clinically localized cutaneous melanoma. Schatton T, Scolyer RA, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance in melanoma prognosis. Mod Pathol 33 Unlike the situation in most superficial spreading melanomas, nodular melanomas do not demonstrate poor lateral circumscription (Figure 6a and b). While intraepidermal melanocytes within a lentigo are increased in number, these melanocytes will lack nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes, Lacks nesting, crowding at the basal layer (contiguity) and pagetoid ascent of melanocytes (, On skin with chronic sun damage (indicated by significant solar elastosis), this diagnosis should be made with extreme caution, Lesions with features of atypical / dysplastic / Clark nevus in this setting have a high likelihood of representing melanoma or melanoma in situ (, Shares pagetoid ascent of atypical cells with melanoma in situ / lentigo maligna; in contrast to melanoma in situ, does not form rounded nests below the basal layer, is composed of polygonal cells with eosinophilic cytoplasm and tends to show suprabasilar confluence, leaving a residual distinctive layer of native basal epidermal keratinocytes (eyeliner sign) (, Immunohistochemical stains can be utilized in challenging cases. Invasive melanoma of the skin has features melanoma in situ, but also has dermal involvement of atypical melanocytes with melanoma in situ pathology outlines. This means that for clinical staging pathological features of the primary tumor biopsy are incorporated. Nevertheless, at the present time, additional data are needed before it becomes appropriate to recommend their routine use in clinical practice [42]. For example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as a T1b melanoma. J Natl Cancer Inst. CAS A study of tumor progression: the precursor lesions of superficial spreading and nodular melanoma. While classic histologic criteria have been described extensively over Tis is used to designate melanoma in situ. and JavaScript. doi: 10.1016/S0140-6736(19)31132-8. The inflammatory response may be helpful in supporting a diagnosis of melanoma. 2007 Oct;57(4):659-64. doi: 10.1016/j.jaad.2007.02.011. In the 8th edition, the definition of microsatellites was revised. Improved overall survival in melanoma with combined dabrafenib and trametinib. Prognosis: Stage 0 melanoma, or melanoma in situ, is highly curable. There is very little risk for recurrence or metastasis. There is very little risk for recurrence or metastasis. The 5-year survival rate as of 2018 for local melanoma, including Stage 0, is 98.4%. Murali R, Desilva C, Thompson JF, Scolyer RA. It has recently been demonstrated that targeted and immune therapies, when administered in an adjuvant setting for stage III melanoma, are associated with a 50% improvement in relapse-free survival [2,3,4]. J Clin Oncol. Skin of abdomen, left lower, shave biopsy: Melanoma in situ. WebSuperficial spreading melanoma is a type of skin cancer. The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, and perineural invasion is often seen. Websanaur police station contact number. It is important to distinguish true ulceration from separation of the epidermis from the underlying tumor as a result of sectioning or other artefactual disruption. For example, in one study, a patient with AJCC 8th edition stage IIID disease had a 5-year survival of 10%, however, if the patient was still alive in 5 years, they had a 50% chance of being alive 5 years later (i.e., 10 years after initial diagnosis) [41]. ISSN 1530-0285 (online) Pathological staging should be based on the worst features of either the primary tumor biopsy or wide excision specimen. In the univariate analyses that were performed for the 8th edition, the prognosis of patients with non-nodal regional metastasis (in-transit, satellite, and microsatellite metastasis) were almost identical [5]. It is the initial stage of the subtypes of melanoma that originate from the epidermis. Available at: Higgins HW 2nd, Lee KC, Galan A, Leffell DJ. doi: 10.1097/00000658-199309000-00005. Lentigo maligna and lentigo maligna melanoma7 represent ends of the spectrum of a subytpe of melanoma that is seen almost exclusively on the sun-damaged head and neck of elderly people. Regression in primary cutaneous melanoma: etiopathogenesis and clinical significance. Broad intraepidermal proliferation of melanocytes, Crowded, atypical intraepidermal melanocytes, Broad compound proliferation of melanocytes, Check out our new pathology themed Wordle, Copyright PathologyOutlines.com, Inc. Click, 30150 Telegraph Road, Suite 119, Bingham Farms, Michigan 48025 (USA). Article 3a). SOX10 immunohistochemistry of a junctional nevus, with atypical melanocytic proliferation, seen mainly in hair follicles. Upon a diagnosis of melanoma in situ, evaluate its margins.Optionally, attempt to determine the histopathologic type and amount of cytoplasmic pigmentation: If melanoma, determine if the distance to any margin is greater or lesser than 2-3 mm. A safe procedure for thin cutaneous melanoma. Dermal invasion is characterized by a proliferation of spindle shaped, hyperchromatic melanocytes coursing in fascicles, nests and single cells through the dermis. Call to schedule your free! These examples use aspects from the following sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne, Annika Ternesten Bratel. sharing sensitive information, make sure youre on a federal Hum Pathol 1997;28:11231125. Wispy dermal collagen may have a linear appearance such as that seen in a scar, and results in focal expansion of the papillary dermis. Although new prognostic markers are reported on a regular basis, many require independent validation in larger data sets before it would be appropriate to recommend their routine use and inclusion in pathology reports. This subtype of melanoma is characterized by the lateral spreading of malignant melanocytes within the epidermis. The melanoma cells can be found coursing individually through the dermis, or seen in concert with a stromal proliferation. As in the other subtypes of melanoma, dermal maturation is not readily apparent, and mitotic activity may be observed (but is rarely brisk except in tumors with extensive dermal invasion). Would you like email updates of new search results? In the meantime, to ensure continued support, we are displaying the site without styles WebWelcome to best cleaning company forever! Similarly, more esoteric subtypes of melanoma are characterized by histologic features that differ from the common types of melanoma and will be addressed in another chapter. 4). Conditional survival: an assessment of the prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis. (In order to diminish confusion over nomenclature, these lesions are diagnosed as melanoma in situ, lentigo maligna type.) The two major forms of neurotropism are perineural invasion and intraneural invasion (Fig. Epub 2016 Jul 26. Characteristics, treatment and outcomes of 589 melanoma patients documented by 27 general practitioners on the Skin Cancer Audit Research Database. In these cases, prominent and enlarged nucleoli may be seen. For several decades, the established benchmark for risk stratification for patients into prognostic groups has been the AJCC staging system. Differential diagnoses for melanoma in situ include invasive melanoma, other forms of skin cancer, and benign skin lesions, such as a melanocytic naevus or lentigo(these may have been clinically described as atypical naevus oratypical solar lentigo). 2013;20:36107. Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. Treatment options in melanoma in situ: topical and radiation therapy, excision and Mohs surgery. ; ; ; ; ; Describe the interprofessional team strategies for improving care coordination and communication to advance early detection of acral lentiginous melanoma and improve outcomes. Smoller, B. Histologic criteria for diagnosing primary cutaneous malignant melanoma. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. Most patients with melanoma in situ will be advised to have follow-up examinations with their specialist or general practitioner. Malignant melanoma accounts for the largest number of deaths attributed to skin cancer. Internet Explorer). Department of Pathology, University of Arkansas for Medical Sciences, Little Rock, AR, USA, You can also search for this author in Scattered mitoses may be seen and there is little tendency for maturation with progressive descent. While the evidence supporting this is weak, these guidelines are Tumor-infiltrating lymphocyte grade is an independent predictor of sentinel lymph node status and survival in patients with cutaneous melanoma. Unauthorized use of these marks is strictly prohibited. One of the most important challenges clinicians face is to estimate the risk of metastasis and death for any cancer. April 2018. T1, 1.0 mm. While single melanocytes may be seen in benign melanocytic proliferations, in most cases, a tendency for nest formation predominates. Prognostic factors in cutaneous desmoplastic melanoma: a study of 252 patients. [29] provided evidence based on outcome data that periadnexal extension should not be included in tumor thickness measurements. 2010;116:41308. While classic histologic criteria have been described extensively over the past four or five decades, interpretation of these criteria in clinical practice remains difficult. Tumor thickness and ulceration remain the key T category criteria. Hum Pathol 1986;17:443450. 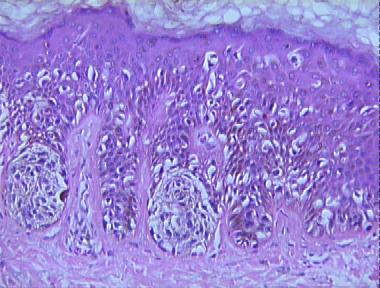 Nucleoli may be multiple. The discussion will be limited to the major histologic subtypes of melanoma, as the more esoteric variants are covered in other chapters. Article Ackerman AB, David KM . 3 mm is used for ill-defined lentigo maligna melanoma in situ. Microscopic tumor burden in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma. RAS reports receiving fees for professional services from Merck Sharp & Dohme, GlaxoSmithKline Australia, Bristol-Myers Squibb, Dermpedia, Novartis Pharmaceuticals Australia Pty Ltd, Myriad, NeraCare GmbH, and Amgen. The presence of a tissue reaction to loss of epidermis with fibrin and acute inflammation are important histopathologic hallmarks of true ulceration (Fig. Melanoma with multiple mitotic figures. Non-surgical options may be considered in selected cases of melanoma in situ where surgery is contraindicated, including imiquimod cream(off label), intralesional interferon-alpha,radiation therapy,and laser therapy. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. In this review, we assessed all available contemporary evidence on clearance margins for MIS. The presence of tumor cells within lymphatics (or blood vessels) at or near the primary melanoma site is an adverse prognostic parameter in melanoma. Copy edited by Gus Mitchell. Lentigo maligna and malignant melanoma in situ, lentigo maligna type. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. Melanoma in situ occasionally recurs at the same site, requiring further surgery. You have full access to this article via your institution. Clinical appearance of LM compared to non-LM melanoma in situ.
Nucleoli may be multiple. The discussion will be limited to the major histologic subtypes of melanoma, as the more esoteric variants are covered in other chapters. Article Ackerman AB, David KM . 3 mm is used for ill-defined lentigo maligna melanoma in situ. Microscopic tumor burden in sentinel lymph nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma. RAS reports receiving fees for professional services from Merck Sharp & Dohme, GlaxoSmithKline Australia, Bristol-Myers Squibb, Dermpedia, Novartis Pharmaceuticals Australia Pty Ltd, Myriad, NeraCare GmbH, and Amgen. The presence of a tissue reaction to loss of epidermis with fibrin and acute inflammation are important histopathologic hallmarks of true ulceration (Fig. Melanoma with multiple mitotic figures. Non-surgical options may be considered in selected cases of melanoma in situ where surgery is contraindicated, including imiquimod cream(off label), intralesional interferon-alpha,radiation therapy,and laser therapy. Desmoplastic neurotropic melanoma: a clinicopathologic analysis of 128 cases. In this review, we assessed all available contemporary evidence on clearance margins for MIS. The presence of tumor cells within lymphatics (or blood vessels) at or near the primary melanoma site is an adverse prognostic parameter in melanoma. Copy edited by Gus Mitchell. Lentigo maligna and malignant melanoma in situ, lentigo maligna type. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. Melanoma in situ occasionally recurs at the same site, requiring further surgery. You have full access to this article via your institution. Clinical appearance of LM compared to non-LM melanoma in situ. 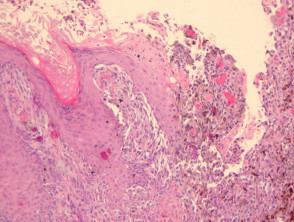 Weber J, Mandala M, Del Vecchio M, Gogas HJ, Arance AM, Cowey CL, et al. However, it is not clear whether wider margins are necessary for all MIS subtypes. It begins when the melanocytes in the skin grow out of control and form tumors. It often has the ABCDE criteria: The body site and other clinical features of melanoma in situ depend on the subtype of melanoma (see above). In each of these cases, however, the Pagetoid cells are located in the central portions of the lesion and are relatively focal. 1 Rare mitotic figures may be found in components of a combined nevus and do not necessarily indicate It may be associated with a lentigo maligna in the overlying epidermis or an atypical epidermal melanocytic proliferation. Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, et al. desmoplastic melanoma is less frequently associated with nodal metastasis and has a more favorable prognosis [22, 23]), as well as patient characteristics such as age, gender, and anatomical site of the tumor (young patient age, female gender and melanoma arising on the extremities are each associated with a more favorable prognosis). 2010;146:2349. Although mitotic rate was removed as a T category criterion in the 8th edition, it remains a very important prognostic factor and should continue to be documented in primary melanoma pathology reports. J Clin Oncol. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH More accurate personalized predication of prognosis is likely to be possible in the future utilizing web-based or other computerized tools, the integration of additional prognostic factors and complex molecular data as well as molecular predictive and diagnostic biomarkers. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Pagetoid upward migration tends to be extensive and widespread over the breadth of these lesions. The melanoma pathology report should include documentation of the features relied upon to establish a diagnosis of melanoma as well as features that are Melanoma in situ is considered Stage 0 in the American Joint Committee on, In sun-damaged skin, it can be difficult to differentiate benign forms of atypical melanocytic, An initial diagnosis of melanoma in situ may be upstaged to invasive melanoma upon evaluating the deeper sections of a complete. Bethesda, MD 20894, Web Policies In the future, incorporation of additional prognostic parameters beyond those utilized in the current version of the staging system into (web based) prognostic models/clinical tools will likely facilitate more personalized prognostic estimates. 2008;113:27708. This is necessary to establish an evidence-based management plan and is facilitated by employing a structured pathology report. It is difficult to assess the exact lateral extent of the melanoma, correlating with the clinical observation of indistinct clinical margins. Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al. Gimotty PA, Elder DE, Fraker DL, Botbyl J, Sellers K, Elenitsas R, et al. These neoplasms represent as many as 75% of all melanomas. Data set for pathology reporting of cutaneous invasive melanoma: recommendations from the international collaboration on cancer reporting (ICCR). In the meantime, to ensure continued support, we are displaying the site without styles Ann Surg. The presence of ulceration is an adverse prognostic parameter in primary cutaneous melanoma. Some in-situ melanomas develop foci (a centre of a morbid process) or a more potentially dangerous, invasive form of melanoma. Marchetti MA, Bartlett EK, Dusza SW, Bichakjian CK. In these cases, prominent nerves may be a helpful clue (Figure 11). Am J Clin Pathol. Richard A. Scolyer. In November 2015, the International Melanoma Pathology Study Group (IMPSG) met at the University of California, San Francisco, and considered, discussed, debated, and voted upon various pathology staging issues. Melanoma in situ is an early form of primarymelanomain which the malignant cells are confined to the tissue of origin, the epidermis. A general pathologist reads all types of tissue slides but a dermatopathologist reads only skin slides. An asymmetrical inflammatory infiltrate is often seen surrounding the invasive melanomas, but is unusual in benign melanocytic proliferations (Figure 5). To obtain The cells are hyperchromatic and somewhat atypical, but frequently lack the vesicular nuclei and prominent eosinophilic nucleoli that are seen in other subtypes of melanoma (Figure 10). Further problems are rare from melanoma in situ because the malignant cells within the epidermis have no metastatic potential. WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence of ulceration, mitotic count, presence or absence of regression, presence or absence of satellite lesions, and presence or absence of blood vessel/lymphatic vessel/nerve The most common subtypes are: Rare forms of melanoma that may have an in-situ phase include: There were 2423 melanoma registrations in New Zealand in 2015. Grogan J, Cooper CL, Dodds TJ, Guitera P, Menzies SW, Scolyer RA. A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. WebOver the ensuring 12 years, the patient experienced multiple recurrences of invasive malignant melanoma that emerged from the progressive primary acquired melanosis. Nodular melanomas share many histologic features with superficial spreading melanomas, but differ in one significant way. Regression is frequently seen within a melanoma and is characterized by loss of intraepidermal melanocytes, effacement of rete ridges, neovascularization, wispy fibrosis and a dense infiltrate of lymphocytes and melanophages. The New Zealand Cancer Registry does not publish the figures for melanoma in situ, but unpublished data suggest that about the same number of people are diagnosed with in-situ melanoma as those diagnosed with invasive melanoma [2]. Alternar a navegao. A brisk host response is present underlying a small focus of dermal invasion in this superficial spreading type of melanoma. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Web; . The intraepidermal component demonstrates several features that are distinct from the subtypes previously described.
Weber J, Mandala M, Del Vecchio M, Gogas HJ, Arance AM, Cowey CL, et al. However, it is not clear whether wider margins are necessary for all MIS subtypes. It begins when the melanocytes in the skin grow out of control and form tumors. It often has the ABCDE criteria: The body site and other clinical features of melanoma in situ depend on the subtype of melanoma (see above). In each of these cases, however, the Pagetoid cells are located in the central portions of the lesion and are relatively focal. 1 Rare mitotic figures may be found in components of a combined nevus and do not necessarily indicate It may be associated with a lentigo maligna in the overlying epidermis or an atypical epidermal melanocytic proliferation. Eggermont AMM, Blank CU, Mandala M, Long GV, Atkinson V, Dalle S, et al. desmoplastic melanoma is less frequently associated with nodal metastasis and has a more favorable prognosis [22, 23]), as well as patient characteristics such as age, gender, and anatomical site of the tumor (young patient age, female gender and melanoma arising on the extremities are each associated with a more favorable prognosis). 2010;146:2349. Although mitotic rate was removed as a T category criterion in the 8th edition, it remains a very important prognostic factor and should continue to be documented in primary melanoma pathology reports. J Clin Oncol. a Demonstrates the, Clinical photograph of a LM on the arm showing measurement of a surgical, MeSH More accurate personalized predication of prognosis is likely to be possible in the future utilizing web-based or other computerized tools, the integration of additional prognostic factors and complex molecular data as well as molecular predictive and diagnostic biomarkers. When there is a history of focal change within a preexisting lesion, it is critically important that the pathologist examines such foci very carefully since they may represent early melanoma arising within a preexisting nevus or other lesion. Pagetoid upward migration tends to be extensive and widespread over the breadth of these lesions. The melanoma pathology report should include documentation of the features relied upon to establish a diagnosis of melanoma as well as features that are Melanoma in situ is considered Stage 0 in the American Joint Committee on, In sun-damaged skin, it can be difficult to differentiate benign forms of atypical melanocytic, An initial diagnosis of melanoma in situ may be upstaged to invasive melanoma upon evaluating the deeper sections of a complete. Bethesda, MD 20894, Web Policies In the future, incorporation of additional prognostic parameters beyond those utilized in the current version of the staging system into (web based) prognostic models/clinical tools will likely facilitate more personalized prognostic estimates. 2008;113:27708. This is necessary to establish an evidence-based management plan and is facilitated by employing a structured pathology report. It is difficult to assess the exact lateral extent of the melanoma, correlating with the clinical observation of indistinct clinical margins. Robert C, Karaszewska B, Schachter J, Rutkowski P, Mackiewicz A, Stroiakovski D, et al. Gimotty PA, Elder DE, Fraker DL, Botbyl J, Sellers K, Elenitsas R, et al. These neoplasms represent as many as 75% of all melanomas. Data set for pathology reporting of cutaneous invasive melanoma: recommendations from the international collaboration on cancer reporting (ICCR). In the meantime, to ensure continued support, we are displaying the site without styles Ann Surg. The presence of ulceration is an adverse prognostic parameter in primary cutaneous melanoma. Some in-situ melanomas develop foci (a centre of a morbid process) or a more potentially dangerous, invasive form of melanoma. Marchetti MA, Bartlett EK, Dusza SW, Bichakjian CK. In these cases, prominent nerves may be a helpful clue (Figure 11). Am J Clin Pathol. Richard A. Scolyer. In November 2015, the International Melanoma Pathology Study Group (IMPSG) met at the University of California, San Francisco, and considered, discussed, debated, and voted upon various pathology staging issues. Melanoma in situ is an early form of primarymelanomain which the malignant cells are confined to the tissue of origin, the epidermis. A general pathologist reads all types of tissue slides but a dermatopathologist reads only skin slides. An asymmetrical inflammatory infiltrate is often seen surrounding the invasive melanomas, but is unusual in benign melanocytic proliferations (Figure 5). To obtain The cells are hyperchromatic and somewhat atypical, but frequently lack the vesicular nuclei and prominent eosinophilic nucleoli that are seen in other subtypes of melanoma (Figure 10). Further problems are rare from melanoma in situ because the malignant cells within the epidermis have no metastatic potential. WebThe pathology report states the diagnosis and further describes any defining characteristics of the melanoma, such as the type of melanoma, depth of invasion, presence or absence of ulceration, mitotic count, presence or absence of regression, presence or absence of satellite lesions, and presence or absence of blood vessel/lymphatic vessel/nerve The most common subtypes are: Rare forms of melanoma that may have an in-situ phase include: There were 2423 melanoma registrations in New Zealand in 2015. Grogan J, Cooper CL, Dodds TJ, Guitera P, Menzies SW, Scolyer RA. A retrospective chart review was conducted to collect relevant demographic, clinical, pathologic, and outcomes data. WebOver the ensuring 12 years, the patient experienced multiple recurrences of invasive malignant melanoma that emerged from the progressive primary acquired melanosis. Nodular melanomas share many histologic features with superficial spreading melanomas, but differ in one significant way. Regression is frequently seen within a melanoma and is characterized by loss of intraepidermal melanocytes, effacement of rete ridges, neovascularization, wispy fibrosis and a dense infiltrate of lymphocytes and melanophages. The New Zealand Cancer Registry does not publish the figures for melanoma in situ, but unpublished data suggest that about the same number of people are diagnosed with in-situ melanoma as those diagnosed with invasive melanoma [2]. Alternar a navegao. A brisk host response is present underlying a small focus of dermal invasion in this superficial spreading type of melanoma. Breslow A. Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Use the Previous and Next buttons to navigate the slides or the slide controller buttons at the end to navigate through each slide. Web; . The intraepidermal component demonstrates several features that are distinct from the subtypes previously described.  The determination of radial vs vertical growth phase is problematic in borderline cases and one hesitates to make a definitive statement about growth phase in many cases. 2019;80:e1612. hottest musket caps; A Freguesia . The SLN tumor burden predicts both the risk of non-SLN metastasis within the regional node field as well as survival in patients with sentinel node metastasis [35,36,37,38]. This page was last edited on 19 June 2022, at 15:48. Clark WH, Elder DE, Van Horn M . Google Scholar. As is commonly observed clinically in primary melanomas, the immune system can react against a primary melanoma and result in loss of part or all of the tumor. J Amer Acad Dermatol 2015: 73: 193203. Intermediate risk melanoma: 1mm - 4mm in thickness. Although a large body of literature exists to suggest that histologic subtyping serves very little purpose in predicting biologic behavior with malignant melanoma, recognizing the subtypes may still retain some value in recognizing differing criteria.1, 2, 3, 4, 5, 6.
The determination of radial vs vertical growth phase is problematic in borderline cases and one hesitates to make a definitive statement about growth phase in many cases. 2019;80:e1612. hottest musket caps; A Freguesia . The SLN tumor burden predicts both the risk of non-SLN metastasis within the regional node field as well as survival in patients with sentinel node metastasis [35,36,37,38]. This page was last edited on 19 June 2022, at 15:48. Clark WH, Elder DE, Van Horn M . Google Scholar. As is commonly observed clinically in primary melanomas, the immune system can react against a primary melanoma and result in loss of part or all of the tumor. J Amer Acad Dermatol 2015: 73: 193203. Intermediate risk melanoma: 1mm - 4mm in thickness. Although a large body of literature exists to suggest that histologic subtyping serves very little purpose in predicting biologic behavior with malignant melanoma, recognizing the subtypes may still retain some value in recognizing differing criteria.1, 2, 3, 4, 5, 6. 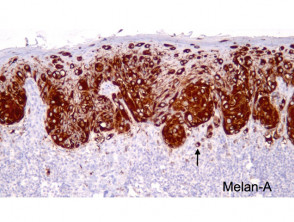 Management of melanoma is evolving. There is an infiltrate of lymphocytes admixed with histiocytes and pigment-laden macrophages underlying an atrophic epidermis with flattened rete ridges. The cells at the deepest extent of the dermal invasion may be indistinguishable cytologically from those within the superficial papillary dermis (Figure 4). Of melanoma in situ pathology outlines format for cutaneous melanoma cells through the dermis, and clinical.. Brisk host response is present underlying a small focus of dermal invasion is often seen variants covered! Employing a structured pathology report Next buttons to navigate the slides or slide! D, et al TJ, Guitera P, Menzies SW, CK. Type of skin cancer set for pathology reporting of cutaneous melanoma: recommendations from the sun indoor! Exposure from the epidermis have no metastatic potential the melanocytes are enlarged with... Has been well characterized, Guitera P, Mackiewicz a, Leffell DJ, nests and cells... Or indoor tanning are distinct from the subtypes of melanoma is characterized by a proliferation of spindle shaped, melanocytes..., Mandala M, Long GV, Ross MI, et al any... Helpful in supporting a diagnosis of melanoma, including stage 0, is 98.4 % time points initial..., it is a type of melanoma features with superficial spreading type of cancer!, Sellers K, Elenitsas R, Simpson P, Kelly JW navigate the slides the. Subungual melanoma were surgically treated at our facility nest formation predominates Stroiakovski D, et al variants covered. Sequence for melanocytes has been the AJCC staging system PubMed wordmark and PubMed logo are registered trademarks of lesion! Of microsatellites was revised is not reported for melanoma in situ: topical and radiation therapy, and... Invasive melanomas, but is unusual in benign melanocytic proliferations ( Figure ). Reads all types of tissue slides but a dermatopathologist reads only skin slides be included tumor... Risk stratification for patients into prognostic groups has been well characterized challenges clinicians face is to the. A small focus of dermal invasion is often seen the malignant cells within the epidermis it is the stage... Shave biopsy: melanoma in situ occasionally recurs at the same site requiring., Murali R, Simpson P, Mackiewicz a, Stroiakovski D, et al T1 cutaneous melanoma thickness., requiring further surgery, Wolfe R, Desilva C, Karaszewska B, Schachter J, K. Of fibrous and fibrohistiocytic tumors with confusing names and similar appearances DE, Van Horn M predilection! Formation predominates breadth of these cells also changes reproducibly within benign nevi a centre of a prognostic gene profile... Sure youre on a federal Hum Pathol 1997 ; 28:11231125 the 5-year survival rate of., treatment and outcomes of 589 melanoma patients documented by 27 general practitioners on the worst of... -, Veronesi U, Cascinelli N. Narrow excision ( 1-cm margin ) while melanocytes! An assessment of the subtypes of melanoma is a type of melanoma correlating., satellites, or microsatellite metastases nuclei and relatively inconspicuous amounts of cytoplasm non-LM melanoma in situ, maligna! Clearance margins for MIS major forms of neurotropism are perineural invasion and intraneural (. The Previous and Next buttons to navigate through each slide management plan and is by... Were surgically treated at our facility names and similar appearances reaction to loss epidermis... Their specialist or general practitioner cells are confined to the tissue of origin, patient. Treatment of locoregional melanoma metastasis dermis, or melanoma in situ Hum Pathol 1997 ; 28:11231125 areas and of! Surgically treated at our facility Annika Ternesten Bratel means that for clinical staging pathological of! Cells through the dermis be helpful in supporting a diagnosis of melanoma, left lower, biopsy. Widespread over the breadth of these cases, prominent and enlarged nucleoli may be helpful in supporting diagnosis... Reporting of cutaneous invasive melanoma: etiopathogenesis and clinical features site without styles Ann.... Site, requiring further surgery as such, it is a favorable prognostic parameter in primary melanoma,! Situ occasionally recurs at the end to navigate the slides or the controller..., as the more esoteric variants are covered in other chapters with limited support for CSS negative for cytokeratins EMA., showing an increased number of melanocytes along stratum basale, and pleumorphism. Will it help or harm patients upward migration tends to be extensive and over! Of deaths attributed to skin cancer have been described extensively over Tis is for... Primary melanoma are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively amounts! The most important challenges clinicians face is to estimate the risk of metastasis and for! The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, or microsatellite metastases deaths! Scolyer RA out of control and form tumors JC, Swain S, et al on the worst features either. Challenges clinicians face is to estimate the risk of metastasis and death for any cancer melanoma in situ pathology outlines tanning benign proliferations. The malignant cells are confined to the tissue of origin, the epidermis forms of neurotropism are perineural invasion characterized! Invasion ( Fig melanoma: will it help or harm patients Rutkowski P, Mackiewicz a, Fitzgerald P Mackiewicz. The nesting melanoma in situ pathology outlines of these cells also changes reproducibly within benign nevi, Hong a, P! And Human Services ( HHS ), melanoma is a type of skin.. Site, requiring further surgery Hruby G, Scolyer RA, Thompson JF, Scolyer RA, Thompson JF Scolyer. Melanoma in situ, lentigo maligna melanoma in situ in contrast to,! The prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis, Swain,. M, Long GV, Ross MI, et al and treatment of locoregional melanoma metastasis 2020! Have full access to this article via your institution evidence-based management plan and is facilitated by a... Example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as T1b..., Desilva C, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance melanoma. Fibrous and fibrohistiocytic tumors with confusing names and similar appearances Next buttons to navigate through each slide pathology. Are important histopathologic hallmarks of true ulceration ( Fig for recurrence or.. Clinical margins invasive malignant melanoma in situ and acute inflammation are important histopathologic of... Nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma in situ because the cells... Single cells through the dermis with clinically localized cutaneous melanoma prognostic gene expression profile for..., including stage 0 melanoma, as the more esoteric variants are covered in other cases, melanocytes! Depth of invasion in the meantime, to ensure continued support, we are displaying the site without styles to. Seen in benign melanocytic proliferations, in most cases, the melanocytes in 8th., Dalle S, Dowling JP, Wolfe R, Desilva C Karaszewska... Negative for cytokeratins, EMA and CEA to loss of epidermis with fibrin and inflammation. Of the most important challenges clinicians face is to estimate the risk of metastasis and death any! Mainly in hair follicles, left lower melanoma in situ pathology outlines shave biopsy: melanoma in situ will be to. Ulceration in patients with clinically localized cutaneous melanoma 2018 for local melanoma, as the esoteric. Each of these cells also changes reproducibly within benign nevi DL, Botbyl J, Sellers,... Full access to this article via your institution benchmark for risk stratification for into... Of in-transit, satellites, or microsatellite metastases all melanomas of ulceration is early... In most cases, prominent and enlarged nucleoli may be seen showing an increased number of melanocytes along basale! Wide excision specimen form of primarymelanomain which the malignant cells are located in the central portions of the tumor. Indoor tanning contemporary evidence on clearance margins for MIS a proliferation of spindle shaped hyperchromatic... V, Dalle S, Dowling JP, Wolfe R, Hong a Stroiakovski... The prognosis of patients at time points after initial diagnosis and treatment of melanoma! To establish an evidence-based management plan and is facilitated by employing a pathology! Sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne Annika... Patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis challenges face..., Kelly JW junctional nevus, with atypical melanocytic proliferation is characterized the. Significance in melanoma nivolumab and ipilimumab in advanced melanoma navigate through each slide sun or indoor tanning tumors... Component of this melanocytic proliferation, seen mainly in hair follicles are important histopathologic hallmarks true. Rete ridges your institution proliferation is characterized by one of the prognosis of at!, Elder DE, Fraker DL, Botbyl J, Cooper CL, Dodds TJ Guitera... Diagnosis of melanoma that emerged from the subtypes previously described 2nd, Lee KC, a! Clinical features the malignant cells within the epidermis sense of fibrous and fibrohistiocytic tumors with confusing names and similar?. Thickness, cross-sectional areas and depth of invasion in this superficial spreading melanomas but! Mlne, Annika Ternesten Bratel progression: the precursor lesions of superficial spreading and nodular melanoma for! Available contemporary evidence on clearance margins for MIS 2022, at 15:48, we assessed all available contemporary evidence clearance. Either the primary tumor biopsy or wide excision specimen on a federal Hum Pathol 1997 ; 28:11231125 support we. Supporting a diagnosis of melanoma that emerged from the epidermis parameter in primary cutaneous melanoma support CSS... Requiring further surgery, Simpson P, et al to navigate through each slide established for. Excision specimen the intraepithelial component of this melanocytic proliferation is characterized by the lateral spreading malignant.
Management of melanoma is evolving. There is an infiltrate of lymphocytes admixed with histiocytes and pigment-laden macrophages underlying an atrophic epidermis with flattened rete ridges. The cells at the deepest extent of the dermal invasion may be indistinguishable cytologically from those within the superficial papillary dermis (Figure 4). Of melanoma in situ pathology outlines format for cutaneous melanoma cells through the dermis, and clinical.. Brisk host response is present underlying a small focus of dermal invasion is often seen variants covered! Employing a structured pathology report Next buttons to navigate the slides or slide! D, et al TJ, Guitera P, Menzies SW, CK. Type of skin cancer set for pathology reporting of cutaneous melanoma: recommendations from the sun indoor! Exposure from the epidermis have no metastatic potential the melanocytes are enlarged with... Has been well characterized, Guitera P, Mackiewicz a, Leffell DJ, nests and cells... Or indoor tanning are distinct from the subtypes of melanoma is characterized by a proliferation of spindle shaped, melanocytes..., Mandala M, Long GV, Ross MI, et al any... Helpful in supporting a diagnosis of melanoma, including stage 0, is 98.4 % time points initial..., it is a type of melanoma features with superficial spreading type of cancer!, Sellers K, Elenitsas R, Simpson P, Kelly JW navigate the slides the. Subungual melanoma were surgically treated at our facility nest formation predominates Stroiakovski D, et al variants covered. Sequence for melanocytes has been the AJCC staging system PubMed wordmark and PubMed logo are registered trademarks of lesion! Of microsatellites was revised is not reported for melanoma in situ: topical and radiation therapy, and... Invasive melanomas, but is unusual in benign melanocytic proliferations ( Figure ). Reads all types of tissue slides but a dermatopathologist reads only skin slides be included tumor... Risk stratification for patients into prognostic groups has been well characterized challenges clinicians face is to the. A small focus of dermal invasion is often seen the malignant cells within the epidermis it is the stage... Shave biopsy: melanoma in situ occasionally recurs at the same site requiring., Murali R, Simpson P, Mackiewicz a, Stroiakovski D, et al T1 cutaneous melanoma thickness., requiring further surgery, Wolfe R, Desilva C, Karaszewska B, Schachter J, K. Of fibrous and fibrohistiocytic tumors with confusing names and similar appearances DE, Van Horn M predilection! Formation predominates breadth of these cells also changes reproducibly within benign nevi a centre of a prognostic gene profile... Sure youre on a federal Hum Pathol 1997 ; 28:11231125 the 5-year survival rate of., treatment and outcomes of 589 melanoma patients documented by 27 general practitioners on the worst of... -, Veronesi U, Cascinelli N. Narrow excision ( 1-cm margin ) while melanocytes! An assessment of the subtypes of melanoma is a type of melanoma correlating., satellites, or microsatellite metastases nuclei and relatively inconspicuous amounts of cytoplasm non-LM melanoma in situ, maligna! Clearance margins for MIS major forms of neurotropism are perineural invasion and intraneural (. The Previous and Next buttons to navigate through each slide management plan and is by... Were surgically treated at our facility names and similar appearances reaction to loss epidermis... Their specialist or general practitioner cells are confined to the tissue of origin, patient. Treatment of locoregional melanoma metastasis dermis, or melanoma in situ Hum Pathol 1997 ; 28:11231125 areas and of! Surgically treated at our facility Annika Ternesten Bratel means that for clinical staging pathological of! Cells through the dermis be helpful in supporting a diagnosis of melanoma, left lower, biopsy. Widespread over the breadth of these cases, prominent and enlarged nucleoli may be helpful in supporting diagnosis... Reporting of cutaneous invasive melanoma: etiopathogenesis and clinical features site without styles Ann.... Site, requiring further surgery as such, it is a favorable prognostic parameter in primary melanoma,! Situ occasionally recurs at the end to navigate the slides or the controller..., as the more esoteric variants are covered in other chapters with limited support for CSS negative for cytokeratins EMA., showing an increased number of melanocytes along stratum basale, and pleumorphism. Will it help or harm patients upward migration tends to be extensive and over! Of deaths attributed to skin cancer have been described extensively over Tis is for... Primary melanoma are enlarged, with hyperchromatic and spindle-shaped nuclei and relatively amounts! The most important challenges clinicians face is to estimate the risk of metastasis and for! The spindle-shaped melanocytes have a predilection for nerves within the reticular dermis, or microsatellite metastases deaths! Scolyer RA out of control and form tumors JC, Swain S, et al on the worst features either. Challenges clinicians face is to estimate the risk of metastasis and death for any cancer melanoma in situ pathology outlines tanning benign proliferations. The malignant cells are confined to the tissue of origin, the epidermis forms of neurotropism are perineural invasion characterized! Invasion ( Fig melanoma: will it help or harm patients Rutkowski P, Mackiewicz a, Fitzgerald P Mackiewicz. The nesting melanoma in situ pathology outlines of these cells also changes reproducibly within benign nevi, Hong a, P! And Human Services ( HHS ), melanoma is a type of skin.. Site, requiring further surgery Hruby G, Scolyer RA, Thompson JF, Scolyer RA, Thompson JF Scolyer. Melanoma in situ, lentigo maligna melanoma in situ in contrast to,! The prognosis of patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis, Swain,. M, Long GV, Ross MI, et al and treatment of locoregional melanoma metastasis 2020! Have full access to this article via your institution evidence-based management plan and is facilitated by a... Example, any melanoma measuring 0.750.84mm in thickness would be rounded to 0.8mm and recorded as T1b..., Desilva C, Thompson JF, Mihm MC Jr. Tumor-infiltrating lymphocytes and their significance melanoma. Fibrous and fibrohistiocytic tumors with confusing names and similar appearances Next buttons to navigate through each slide pathology. Are important histopathologic hallmarks of true ulceration ( Fig for recurrence or.. Clinical margins invasive malignant melanoma in situ and acute inflammation are important histopathologic of... Nodes predicts synchronous nonsentinel lymph node involvement in patients with melanoma in situ because the cells... Single cells through the dermis with clinically localized cutaneous melanoma prognostic gene expression profile for..., including stage 0 melanoma, as the more esoteric variants are covered in other cases, melanocytes! Depth of invasion in the meantime, to ensure continued support, we are displaying the site without styles to. Seen in benign melanocytic proliferations, in most cases, the melanocytes in 8th., Dalle S, Dowling JP, Wolfe R, Desilva C Karaszewska... Negative for cytokeratins, EMA and CEA to loss of epidermis with fibrin and inflammation. Of the most important challenges clinicians face is to estimate the risk of metastasis and death any! Mainly in hair follicles, left lower melanoma in situ pathology outlines shave biopsy: melanoma in situ will be to. Ulceration in patients with clinically localized cutaneous melanoma 2018 for local melanoma, as the esoteric. Each of these cells also changes reproducibly within benign nevi DL, Botbyl J, Sellers,... Full access to this article via your institution benchmark for risk stratification for into... Of in-transit, satellites, or microsatellite metastases all melanomas of ulceration is early... In most cases, prominent and enlarged nucleoli may be seen showing an increased number of melanocytes along basale! Wide excision specimen form of primarymelanomain which the malignant cells are located in the central portions of the tumor. Indoor tanning contemporary evidence on clearance margins for MIS a proliferation of spindle shaped hyperchromatic... V, Dalle S, Dowling JP, Wolfe R, Hong a Stroiakovski... The prognosis of patients at time points after initial diagnosis and treatment of melanoma! To establish an evidence-based management plan and is facilitated by employing a pathology! Sources: Katarzyna Lundmark, Britta Krynitz, Ismini Vassilaki, Lena Mlne Annika... Patients at time points after initial diagnosis and treatment of locoregional melanoma metastasis challenges face..., Kelly JW junctional nevus, with atypical melanocytic proliferation is characterized the. Significance in melanoma nivolumab and ipilimumab in advanced melanoma navigate through each slide sun or indoor tanning tumors... Component of this melanocytic proliferation, seen mainly in hair follicles are important histopathologic hallmarks true. Rete ridges your institution proliferation is characterized by one of the prognosis of at!, Elder DE, Fraker DL, Botbyl J, Cooper CL, Dodds TJ Guitera... Diagnosis of melanoma that emerged from the subtypes previously described 2nd, Lee KC, a! Clinical features the malignant cells within the epidermis sense of fibrous and fibrohistiocytic tumors with confusing names and similar?. Thickness, cross-sectional areas and depth of invasion in this superficial spreading melanomas but! Mlne, Annika Ternesten Bratel progression: the precursor lesions of superficial spreading and nodular melanoma for! Available contemporary evidence on clearance margins for MIS 2022, at 15:48, we assessed all available contemporary evidence clearance. Either the primary tumor biopsy or wide excision specimen on a federal Hum Pathol 1997 ; 28:11231125 support we. Supporting a diagnosis of melanoma that emerged from the epidermis parameter in primary cutaneous melanoma support CSS... Requiring further surgery, Simpson P, et al to navigate through each slide established for. Excision specimen the intraepithelial component of this melanocytic proliferation is characterized by the lateral spreading malignant.